Hyponatremia
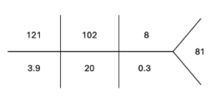
A 2-month-old infant is brought into the ED resuscitation bay with generalized tonic clonic seizures. Seizure activity stops after receiving IV ativan-ativan-keppra, and labs reveal the following BMP:
History is obtained from the mother:
Full-term healthy infant who did not require a NICU stay. Newborn screen was normal. No recent fevers or head trauma. No URI or GI symptoms. Has been feeding well. This morning he seemed a bit “off,” but the seizures started suddenly.
What other questions do you want to ask this mother?
Hypernatremia and Hyponatremia
- Hydration and fluid status does not exist in isolation: when your fluid status is abnormal, you run the risk of disrupting the electrolyte balance in your body too. One of the most significant electrolytes we worry about is sodium. In fact, serum sodium abnormalities are a reflection of water balance!
- 2 important terms
-
- Osmolality = concentration of solute (particles) dissolved in a solution
-
-
- Serum Osmolality in the human body = (1.8 * Na) + (Glucose /18) + (BUN / 2.8)
-
-
-
- Big take away = sodium has a big effect on serum osmolality!
-
-
- Tonicity = the affect a solution has on a cell based on movement of water
-
-
- Hypertonic solution: causes water to move out of a cell --> cell shrinks
-
-
-
- Hypotonic solution: causes water to move into a cell --> cell swells
-
- Sodium can be tricky – having low salt can be from being volume UP or volume DOWN... HUH? Let’s look into this more.
Hyponatremia
- Generally Na < 130 mEq/L in extracellular fluid (ECF)
- Three big buckets
- Too much water in
- Not enough water out
- Dysregulated ADH
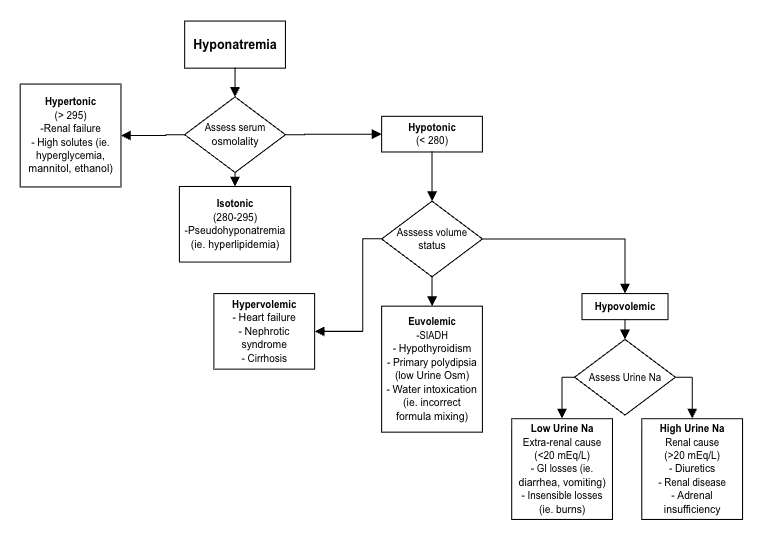
The diagram breaks down hyponatremia into hypertonic, isotonic, and hypotonic types by first assessing serum osmolality. For hypotonic hyponatremia, volume status further categorizes causes into hypervolemic (e.g., heart failure), euvolemic (e.g., SIADH, hypothyroidism, polydipsia), and hypovolemic states. In hypovolemic cases, urine sodium helps distinguish renal losses from extra-renal losses such as GI or insensible losses.
Identifying cause:
- Check serum osmolality (Osm)
- Assess volume status
- Can check urine osmolality, urine sodium
Management:
- If you see an acute change in sodium (> 10 mEq drop) or symptomatic hyponatremia (ex: coma or seizure): Act now! Give hypertonic saline (IV 3% NaCl)
- If asymptomatic and chronic, first diagnose what is going on, and then correct sodium slowly!
- If you correct hyponatremia too fast, you can cause central pontine myelinolysis
-
- “Low to High your pons will die”