Abdominal Pain
Key Conditions
- Core 1 (Pre-Clerkship)
- See Key Conditions
- Core 2 (Clerkship)
- Pediatrics didactic - Acutely Ill
- Surgery
- Pediatric Emergency Medicine Optional Reading: Abdominal Pain and Vomiting, Gastroenteritis, Intussusception, Pyloric Stenosis
- Core 3 (Post-Clerkship)
- Electives that may further knowledge: Pediatric Gastroenterology, Pediatrics Emergency Department
The differential diagnosis of abdominal pain is broad and includes many different organ systems. It is most helpful to think about differential diagnosis of abdominal pain by first deciding if the pain is acute or chronic. The history and physical exam findings will then help to guide the rest of your workup and management. These resources included are not meant to be an exhaustive list of causes of abdominal pain but rather to provide a starting framework of how to think about acute and chronic abdominal pain in the clinical setting.
- Emergency vs. Not Emergency
- Decide based on presence of peritoneal signs on exam, vitals, severity of symptoms/red flags on history
- Develop differential diagnosis based on history and physical exam
- Tailor workup (labs/imaging) based on highest differential diagnoses
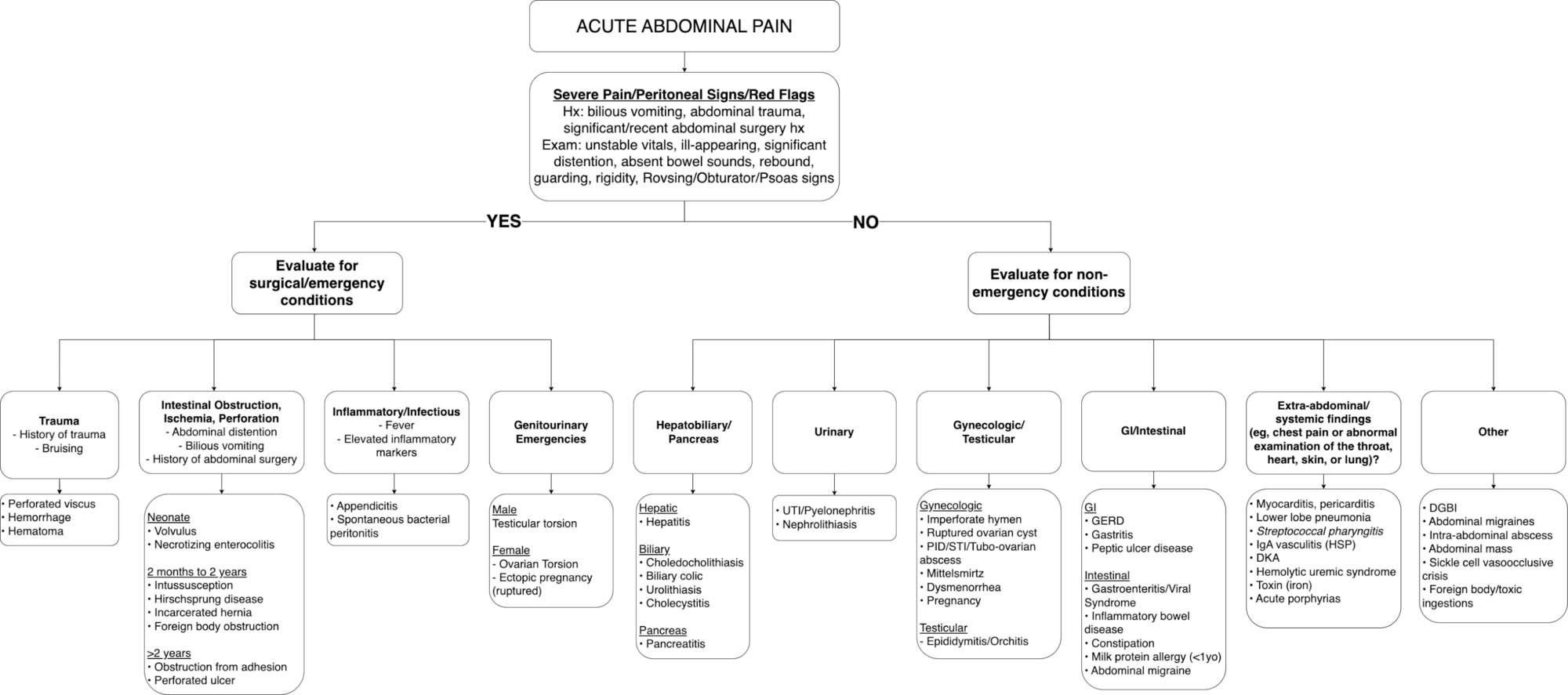
Adapted from: UpToDate Abdominal Pain Algorithm: Males/Premenarchal Females & Postmenarchal Females
A flowchart for evaluating acute abdominal pain in children. It begins with red flags (bilious vomiting, trauma, unstable vitals, distention, peritoneal signs). If yes, evaluate for surgical/emergent causes such as trauma, intestinal obstruction or perforation (with age-based etiologies like NEC, intussusception, adhesions), appendicitis or peritonitis, testicular or ovarian torsion, ectopic pregnancy, hepatitis, biliary disease, and pancreatitis.
If no, evaluate for non-emergent causes including UTI or stones, gynecologic causes (cysts, PID, dysmenorrhea), GI causes (GERD, gastritis, viral gastroenteritis, constipation, IBD, milk protein allergy), systemic/extra-abdominal causes (pneumonia, strep pharyngitis, HSP, DKA, HUS, toxins), and other conditions (DGBI, abdominal migraines, masses, sickle cell crisis, ingestions).
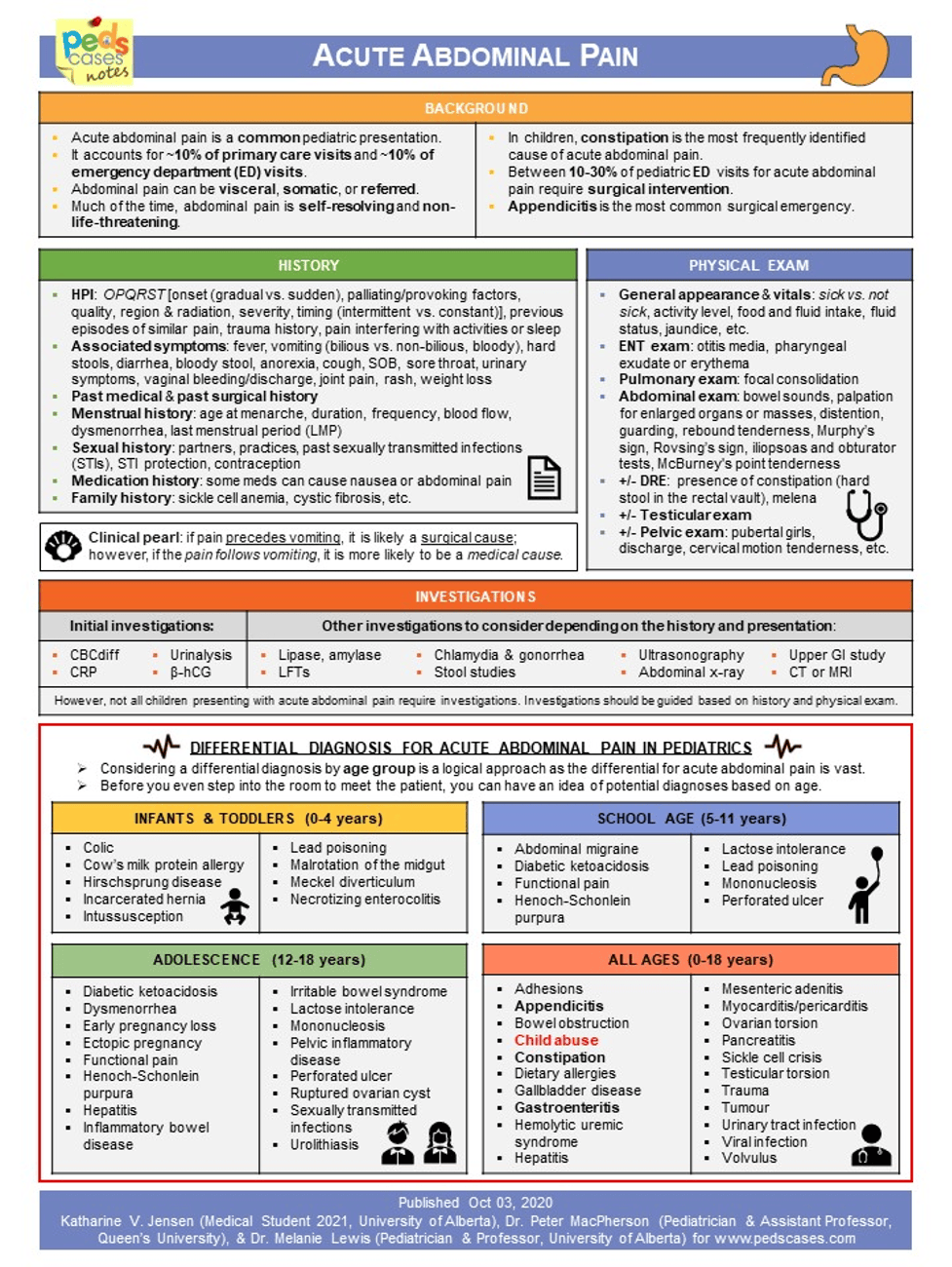
An infographic outlining how to assess acute abdominal pain in pediatrics, covering common causes, red flags, and when to consider surgical emergencies. It highlights important history questions, exam components, and appropriate investigations, and provides a differential diagnosis organized by age group. The bottom section lists conditions ranging from benign (constipation, colic) to urgent (appendicitis, obstruction, ectopic pregnancy).

This infographic presents a stepwise algorithm for assessing acute abdominal pain in children, starting with red flags that warrant surgical consultation, followed by pathways based on symptoms like constipation, diarrhea, urinary issues, pregnancy risk, and respiratory findings. It includes the Pediatric Appendicitis Score with risk-based management guidance and a detailed section on identifying and treating constipation, the most common cause of abdominal pain. A final box highlights important safety points, including when to seek further evaluation and the need for clear return precautions.
Refer to Disorders of Brain Gut Interaction – Key Condition Page for more information
- Evaluate for red flags signs on history or physical exam
- If no red flags, likely DGBI (most common) –> treat!
- If there are red flags concerning for organic etiology –> tailored workup and treatment based on differential
Note: Chronic abdominal pain can evolve into acute complications and may develop red flag symptoms over time. Always re-assess diagnosis of DGBI if symptoms change or if symptoms are refractory/worsening despite appropriate treatment.

This flowchart guides the assessment of chronic abdominal pain by first identifying red flag symptoms such as weight loss, nocturnal pain, bloody stools, systemic signs, or abnormal exam findings. If present, it directs clinicians to evaluate for organic causes across GI, intestinal, hepatobiliary, and genitourinary categories. If red flags are absent, the chart recommends using Rome criteria and a multimodal approach to disorders of gut–brain interaction, including psychotherapy, pelvic PT, lifestyle changes, and medication adjuncts.
Here is a great review video of the skills needed to do a comprehensive pediatric abdominal exam! Some key things to pay attention to on exam are:
- Peritonitic signs: rebound/guarding
- Distention
- Bowel sounds
- Hepatosplenomegaly
- Digital rectal exam: Tone/fissures/tags
- Appendicitis exam maneuvers: McBurney’s point, Psoas sign, Rovsing sign, Obturator sign
- CVA tenderness
- Abdominal Pain Case Document
- Facilitator Guide (Great cases to download and work through with students)
- Student Guide
- Quick Online Abdominal Pain Cases from Peds Cases
- Detailed Abdominal Pain/Mass Case Curriculum
- Abdominal Pain Illness Script Presentation
- Peds Cases One Page Notes for Chalk Talks
- Review self-Assessment Questions
General Resource
Acute Abdominal Pain
- UpToDate Abdominal Pain Algorithm: Males/Premenarchal Females & Postmenarchal Females
Chronic Abdominal Pain